ACT UP FIGHT AIDS
MASK UP FIGHT COVID
Opinion: Is it time for an ACT-UP for Long COVID?
https://48hills.org/2024/10/opinion-is-it-time-for-an-act-up-for-long-covid/
ByBRUCE MIRKEN
OCTOBER 9, 2024
While I’m far from the only person worried about Long COVID and our society’s general inclination to look away and pretend it’s not there, people like me certainly feel badly outnumbered. It’s beginning to feel reminiscent of how people with AIDS and their loved ones felt circa 1986—and maybe it’s time for the same kind of response.
For those of you lucky enough not to have lived through that era, by the end of 1986, AIDS had killed nearly 25,000 Americans, but president Ronald Reagan had yet to speak the word “AIDS.” His press secretary had joked about it and the White House press corps laughed. While individual scientists were doing important work, the bureaucracies running the NIH and FDA seemed very much to be in business-as-usual mode. Because the casualties had largely been gay men and injection drug users, it seemed like no one with any power cared whether we lived or died.
So, a group of New Yorkers – mostly gay men – decided it was time to start raising hell. Calling themselves ACT UP, they disrupted the New York Stock Exchange and, as chapters sprang up nationwide, they staged protests that shut down the FDA and NIH. Eventually, people like Anthony Fauci began to see they had a point. I joined the Los Angeles ACT UP chapter in 1988 and ended up getting arrested half a dozen times in protests at the LA federal building, the County Board of Supervisors and the U.S. Capitol, among others. We won major improvements in HIV/AIDS care in the Los Angeles County health system, which cared for thousands of people with AIDS who had no health insurance. When I landed in San Francisco in 1993, I connected with ACT UP Golden Gate.
I get that COVID has played out very differently than HIV/AIDS. AIDS ramped up slowly and seemed not to affect “normal” people until it killed closeted gay movie and TV star Rock Hudson in 1985, and even then officials largely looked the other way. Only scientific breakthroughs in the 1990s finally stemmed the tide of death. In contrast, the much more highly transmissible SARS-CoV-2 virus came on fast and furious, turning Americans’ lives upside-down almost immediately.
But now, we’ve arrived at what seems in some ways like an eerily similar place. When needed precautions to curb a highly infectious airborne virus spurred frustration and political pushback, officials largely threw up their hands and gave up. Even measures that don’t involve mandates or restrictions on behavior have mostly either been dropped or never happened in the first place.
A RADICAL IDEA: DO WHAT WORKS
We know what to do. As Clean Air Club founder Emily Dupree and co-author Shelby Speier wrote in Sick Times in May, “We possess the technology to make public spaces safer. Studies show HEPA air purification and far-UVC lamps drastically reduce the number of airborne pathogens in a room and therefore lessen the likelihood of COVID-19 transmission. When combined with other layers of protection, these tools have the potential to finally make our shared spaces more accessible during an airborne pandemic.”
A key word here is accessible. Failure to address indoor air quality and other prevention measures makes public spaces seriously dangerous for those at highest risk, including the elderly, the immunocompromised and those with long-term health issues, including Long Covid.
Such simple, factual messages are rarely heard in official statements about COVID. “What I find the most frustrating about official handling of COVID and prevention is the lack of care, education, and honoring the science around COVID,” comments Clear the Air ATX founder and Long Covid activist Katie Drackert. “Telling people to ‘stay home when they feel sick’ for a virus that spreads asymptomatically? Well, they are just straight up ignoring science.”
Admirable as they are, the small, volunteer-driven efforts of groups like Drackert’s and Dupree’s are not remotely comparable to the scale of the problem. For now, people must take matters into their own hands. “In the year 2024, people still need to be wearing a well fitted KN95 or above for optimal communal and individual protection,” Drackert says. In the absence of reliable information about air quality in indoor spaces, she suggests getting a portable air quality monitor, which can be reasonably affordable. “High CO₂ levels indicate poor ventilation, which may lead to higher concentrations of aerosols that could contain the virus,” she explains. “Some air quality monitors track particulate matter (PM2.5 and PM10), which are small airborne particles. While COVID is smaller than these particles, high PM levels may indicate poor indoor air quality.”
Most of us can’t entirely avoid being in spaces with poor air quality, and that leaves us with masking, which the country has largely abandoned. Worse, we’re starting to see bans on face coverings in public spaces being enacted—for example, in Nassau County, New York, and North Carolina.
These laws typically contain exceptions for people masking for health reasons, but, as New Jersey’s Star-Ledger noted in a recent editorial opposing a proposed mask ban, “[I]t leaves it up to the cops to decide whether someone has a legitimate medical reason for wearing a mask at a public gathering.
“How will they know that? It’s subjective. And based on past experience, we know what that means: Police will disproportionately stop and question Black and brown people, who have also been the most likely to continue wearing masks to protect against COVID-19.”
It’s hard to imagine a more demented public policy than making disease prevention illegal. And it’s not hard at all to imagine a COVID-19 prevention framework that would make a meaningful difference without causing a nationwide freakout:
Encourage masking. Even if mask mandates are a political non-starter, there’s still plenty we can do. First, officials can talk about it and actively encourage people to wear high-quality protection like N-95s when in busy, indoor spaces. They can remind people of its importance—that COVID is not over, not just a cold, and that even a “mild” case can change your life forever. Federal, state and local governments could distribute N-95s or KN-95s free or at minimal cost.
Get serious about indoor air purification. Build on what the Biden administration started a few years ago: Develop medically informed, enforceable indoor air quality standards and create a verification system so that people know when a building they enter meets them. Start with public buildings and the largest, busiest private venues, like sports arenas, concert halls and theaters, and move on from there. Give business owners generous technical and financial support in meeting those standards, and a reasonable amount of time in which to do it. While this program is ramping up, fund the local organizations now struggling with limited resources to fill the gap.
None of this is that difficult. It’s not even that expensive when you consider that the federal government is in the process of spending $634 billion to upgrade nuclear weapons that with any luck will never be used. What’s missing is political will, and that won’t be there until people scream bloody murder.
That’s why I think it may be time for a new version of ACT UP focused on COVID-19. The issues are somewhat different, but less so than you might think. While the original ACT UP focused a lot on research, treatment and care, it also addressed prevention. ACT UP chapters around the country started syringe exchange programs, handed out condoms at high schools, and sometimes succeeded in shaming the system into doing the right thing. And of course, there are issues to tackle around Long Covid research that I haven’t addressed here, but which I will try to cover in a future piece.
The fundamental problem is much the same as people with AIDS faced in 1986: a system stuck in neutral, politicians stuck in denial, and a public closing their eyes, covering their ears and shouting, “I don’t hear you!”
The first task must be to break the system–and the broader population, as much as possible–out of its present inertia, complacency and denial.
Masks are community care❤️🔥😷 free masks: maskbloc.org
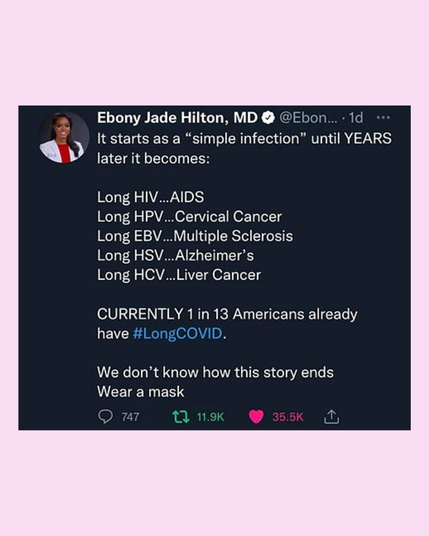
• Remember: covid is not over, 50% of infections are asymptomatic, minimum 10% of infections end up in long COVID, re-infections wreck us, COVID spreads and moves like cigarette smoke, think of the people around you and you as people who are all day smoking, it becomes more visual to understand how COVID moves.
• There is no way to “train” the immune system because it is not a muscle. there is a common misconception that exposure to harmful germs strengthens the immune system. viral diseases like COVID, flu, measles weaken the immune system, leaving the possibility of lasting damage. The reality is that you don't build your immunity with repeated infections, vaccines strengthen the immune system by teaching it to recognize pathogens without all the risks. Focusing on infection prevention is key.
• Rapid antigen tests give many false negatives.
• Solving the pandemic was never in the cards for the capitalist world.
• Instead, the explicit goal of the ruling class has been to make the pandemic simply disappear from public perception. Any reminder of the existence of a highly-transmissible, highly-dangerous, mass-disabling disease could trigger panic, or worse: organized, militant labor action. Averting this crisis required a careful campaign of culture-crafting; the people themselves needed to become convinced that there was no reason to fight. Consent for protracted mass infection needed to be manufactured.
#MaskUp #WearAMask #CovidRealist #CovidIsAirbone #LongCovid #YallMasking #DisabledLiberation #DisabilityJustice
.