Book review: A handbook of learning for transformation
A cartography of learning for transformation
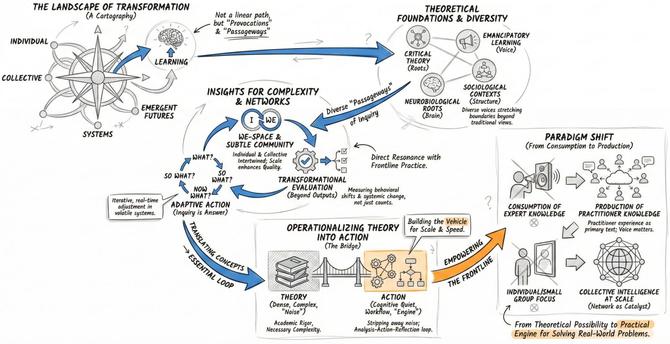
The Palgrave Handbook of Learning for Transformation offers a sweeping map of the territory of transformative learning. The editors have curated a massive collection of perspectives that stretch the boundaries of the field beyond its traditional roots in the work of Jack Mezirow. The volume is organized not as a linear textbook but as a series of provocations that invite the reader to wander through different passageways of inquiry.
As the editors Nicolaides and Eschenbacher explain, “a passage points to two directions – backward to the space one is leaving, and forward to the space one is approaching”. This orientation is critical because it frames the book not as a final destination but as a movement toward something new.
This structure allows for a rich diversity of voices:
Why should busy practitioners engage with this handbook?
As global health and humanitarian practitioners, we often feel the limitations of the transmission models of training that dominate our sector, yet we sometimes lack the precise vocabulary to explain why they fail in our complex, adaptive environments. This handbook is not a quick or easy read. It is dense, academic, and demanding. It is likely best suited for those of us – program designers, strategists, and technical leads – who are willing to wade through significant theoretical weight to find a more robust way forward. If we are willing to make that effort, this volume offers the intellectual grounding necessary to articulate why linear project cycles fall short in volatile crises and why we are more likely to make progress when we prioritize inquiry-based, networked learning. It equips us to defend the shift away from top-down directives toward approaches that center the frontline worker, helping us design evaluation metrics that measure genuine behavioral change rather than simple compliance.
Insights for networked and complex learning for transformation
Three chapters in this volume stand out for their direct resonance with the work of connecting frontline practitioners to solve complex problems. These contributions offer theoretical grounding that can strengthen practices focused on networked learning and collective intelligence.
Chapter 38: The Interpenetration of Individual and Collective Transformation.
Abigail Lynam and her colleagues present a framework that is vital for understanding how learning scales. They argue that individual and collective development are not separate processes but are deeply intertwined. This mirrors the dynamic we observe in large-scale peer networks where the “We” becomes a powerful engine for the growth of the “I.” They describe how the “subtle We” consists of “the perception of being situated in and arising out of a plurality of contexts” where “the We is not then a specific group of people, but is a relational space, a quality brought to relationships, or a relational field”. Their discussion of “subtle community” and the movement from differentiation to integration provides a useful vocabulary for understanding how digital networks can become spaces of profound connection and shared purpose rather than just channels for information exchange.
Chapter 39: Power of Questions: Transformation in Complex Systems.
Glenda Eoyang’s contribution is essential for any organization operating in volatile and uncertain environments. She argues that in complex systems, traditional answers and linear plans often fail. As she states, “Certainty will never be possible, so it must be replaced with inquiry”. Her approach to “Adaptive Action” – asking What, So what, and Now what – aligns perfectly with the need for iterative, action-oriented learning cycles. She notes that “answers are useful only in limited space and over a short period of time”. This chapter validates the move away from didactic training toward inquiry-based models where learners interrogate their own reality. It reinforces the idea that transformation in complex settings requires the ability to see patterns and adjust actions in real time rather than adhering to rigid protocols.
Chapter 44: Evaluation as a Pathway to Transformation.
Scott Chaplowe and his co-authors tackle the critical challenge of measuring impact in complex systems. They critique the industry’s fixation on metrics, citing Natsios to note an “Obsessive Measurement Disorder” where the production of evidence undermines the very interventions it is supposed to support. They vividly illustrate the problem by quoting Mueller: “the snake of accountability eats its own tail”. They propose a shift toward “transformational evaluation” that supports learning and adaptation. This is crucial for organizations that seek to bridge the gap between learning and performance. It suggests that we must move beyond counting the number of people trained to measuring the actual shifts in behavior and the tangible outcomes that result from learning. This chapter provides a robust theoretical basis for measuring impact through the lens of systems change rather than simple compliance.
How does our work connect to the learning and insights of the handbook?
The handbook offers a rich theoretical map. The approach we take at The Geneva Learning Foundation complements this map by building the vehicle required to traverse this territory at speed and scale. While the handbook often focuses on the intimate or the theoretical, our work demonstrates how these principles can be operationalized for thousands of learners simultaneously.
From theoretical complexity to cognitive quiet
The handbook is dense with academic rigor and complex language. Arguably, this complexity may be necessary for the advancement of theory. TGLF’s approach complements this by translating these high-level concepts into cognitive quiet. We strip away the theoretical noise to focus on the essential loop of analysis, action, and reflection. As Eoyang points out, in complex environments, “one simple intervention sets conditions for multiple, unpredictable transformational changes”. We strive to turn sophisticated ideas from learning theory and embed them into simple, accessible workflows that busy professionals can use immediately. We nourish the handbook’s theories by showing they work not just in the seminar room but in the gritty reality of communities facing multiple, intertwined crises.
From individual reflection to collective intelligence
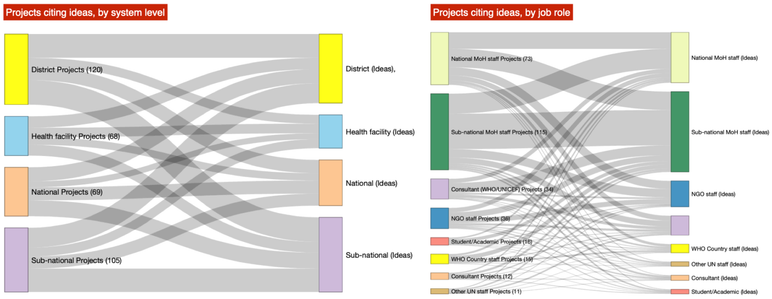
Many chapters in the handbook focus on the individual or small group as the unit of transformation. We expand this horizon by demonstrating that scale enhances quality. The “We-Space” discussed by Lynam need not be limited to a room of people. It can be a digital network of thousands. Fergal Finnegan, in Chapter 4, warns against the “false dichotomy” between individual and social transformation, noting that “it is a mistake to treat collective agency as a simple scaled-up aggregate version of what happens at an individual level”. Our approach is proving that when you connect vast numbers of peers, you generate a collective intelligence that exceeds the capacity of any single room full of experts. We take the theoretical possibility of collective transformation described in the text and turn it into a practical engine for local actors solving real-world problems.
Producing new learning for transformation
The handbook, by its nature, is a collection of expert knowledge to be consumed by the reader. Our work complements this by inverting the model. We treat the learner not as a consumer of the handbook’s wisdom but as a producer of new knowledge. We operationalize the decolonial and emancipatory themes found in the book by centering the experience of the practitioner as the primary text. As Seehawer and colleagues note in Chapter 26, we must move away from focusing on challenges and toward “recognising our agency as teachers and lifelong learners”. The handbook explains why voice matters. Our platform gives that voice a global megaphone. We operationalize the philosophy contained in these pages by building the digital infrastructure that allows the learners themselves to theorize their practice and lead the transformation of their own systems.
Reference
Nicolaides, A., Eschenbacher, S., Buergelt, P., Gilpin-Jackson, Y., Welch, M. and Misawa, M. (Eds.), (2022). The Palgrave handbook of learning for transformation. Palgrave. 956 pp. $279 USD (hardcover), ISBN: 978-3-030-84693-0. https://doi.org/10.1007/978-3-030-84694-7