Implementation science for planetary health
Remarks about implementation science for planetary health by Reda Sadki, Executive Director, The Geneva Learning Foundation at the Centre for Planetary Health’s research corner meeting, London School of Hygiene & Tropical Medicine (LSHTM) on December 17, 2025.
Pauline Paterson (LSHTM): We are really delighted to welcome Reda Sadki. Reda is the Executive Director of the Geneva Learning Foundation, a non-profit research organization developing new epistemological and methodological approaches for complex global health challenges. Welcome, Reda.
Reda Sadki (TGLF): Warm greetings from Geneva, Switzerland. I am very pleased to share with you what we have been learning about climate change and health – in particular, how we can move from ground truth to local action on a global scale.
Since 2021, we have been running an initiative called Teach to Reach, led by community-based health professionals from all over the world. It connects people across countries and job roles, supporting the journey from local insight to global health initiative.
The scale of this network has grown significantly. In March 2021, we started with 2,604 participants. By December 2024, at the eleventh meeting of Teach to Reach, we had 24,610 health workers participating.
Who are they? Most work in health facilities and districts. Half work for government and half for civil society organizations.
Where are they? They serve in the most fragile contexts: 62% work in remote rural areas; 47% with the urban poor; 25% with refugees or internally displaced populations. And one in five work in areas of active armed conflict.
Alongside these individuals, we are nurturing the REACH Network, a coalition of more than 4,000 locally-led organizations. This is the backdrop for how we think about leadership as the key to driving change in climate and health.
The “dark matter” of implementation science
As a community working on climate change and health, we are strong – and getting stronger – on diagnosis. But we must be candid: we are weak on delivery. The science keeps getting better, but there is a gap when it comes to translating science into action.
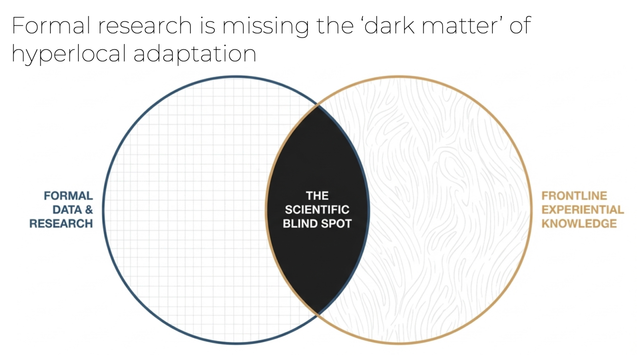
When it comes to formal research, we see what I call the ”dark matter”, a blind spot around hyperlocal adaptation and how implementation actually happens at the local level.
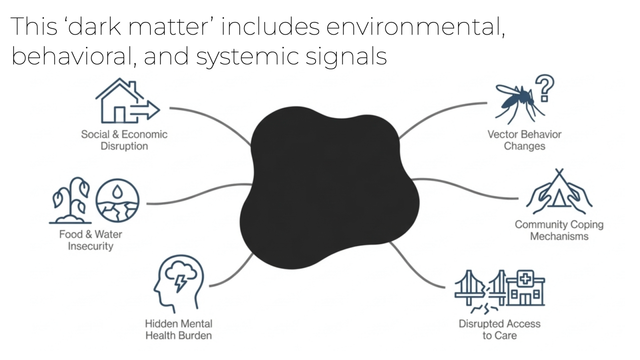
This dark matter includes environmental, behavioral, and systemic signals that formal research might miss: social and economic disruption, hidden mental health burdens in communities with no formal services, community coping mechanisms, and subtle changes in vector behaviors.
Now, I know that for many of you trained in epidemiology, the word “anecdote” sets off alarm bells. We are taught to devalue it for good reason: it is prone to recall bias, selection bias, and lacks denominators. A nurse in Bangladesh noticing “more heatstroke” is a signal, not a prevalence study. We are not claiming it is.
However, we have two ways to answer the questions these signals raise. We can carry out long-term, rigorous academic studies over decades. Or – given that we are past several climate tipping points – we can recognize that aggregate patterns formed by thousands of these signals offer a speed and granularity that traditional studies cannot match. This functions as a massive, distributed sentinel surveillance system. It may be “imperfect” compared to a controlled trial, but is it riskier than the alternative? The alternative is often waiting years for definitive answers while communities suffer damage that may make those findings moot.
This requires a new epistemology. Our hypothesis is that we can build a system where an anecdote becomes an eyewitness report. A health worker, traditionally seen as a “knowledge recipient” presumed ignorant of climate science, becomes a “knowledge creator”. They know things about local impacts that no one else knows, simply because they are there every day.
In July 2023, Charlotte Mbuh, TGLF’s director who started over a decade ago as a sub-national health worker from Cameroon, stood at COP28 and said:
”What we know, we know because we are here every day. We are already managing the impacts of climate change on health. We are doing the best we can, but we need your support.”
Read Charlotte Mbuh’s full statement at COP28: Climate change is a threat to the health of the communities we serve: health workers speak out at COP28
Turning experience into evidence: the global climate change and health survey
To operationalize this, we built a living laboratory powered by a global human sensor network.
In 2025, in partnership with Grand Challenges Canada and a group of 50 global funders (including Gates, Wellcome, and Rockefeller), we conducted what I have been told is the largest-ever climate and health survey, and the one with the highest level of responses from local communities in the most climate-vulnerable regions
We received responses from 6,436 health workers, primarily from the sub-national level. Because of the trust we have built over years, the Teach to Reach network contributed over 60% of these responses, ensuring we heard from the most climate-vulnerable regions.
https://www.youtube.com/watch?v=C67nYqq-hP0
Most importantly for funders, we asked about barriers to action. The top barriers were not just resource shortages, but structural issues.
Pending their formal publications, I am not yet able to share results.
These findings are signals. They generate hypotheses. Here are three examples of hypotheses grounded in health worker experirences:
- Geh Raphaela Agwa, a midwife from Cameroon, told us: “During this unfavourable weather period, people who can paddle canoes come in and help…”. Could community-led transport solutions improve maternal health access during floods?
- Solace Jewel Morgan, a disease control officer in Ghana, told us: “The dry season… results in dust particles known as harmatan. This leads to a high incidence of respiratory illnesses… encourage… free distribution of personal protective masks.” Could prophylactic mask distribution reduces respiratory morbidity during the harmatan season?
- Victoire Odia, a nurse from the Democratic Republic of Congo (DRC), told us that during extreme weather events, maternity “stays were paid for by the women’s group solidarity fund.” Could micro-financing networks increase facility-based deliveries in climate-vulnerable areas?
Of course, we must distinguish between generating a hypothesis and validating an intervention. We do not claim every local idea is safe or effective immediately. But we do claim that listening is the prerequisite to testing them.
From insight to impact: the Accelerator model for implementation science
We do not just extract data. We give it back to the community to prompt action. Since 2016, we have developed an “Accelerator” system that moves from listening to implementation. It works on a simple rhythm: participants set a specific, practical goal on Monday, and on Friday, they report on what happened, receiving feedback from peers.
This brings us to a critical tension: the balance between context and content. Critics might argue that prioritizing “context over content” carries risks. What if health workers implement unproven or suboptimal strategies? That is a valid concern. However, we see this mechanism not as a way to bypass evidence, but as the most effective tool to operationalize it.
In The Geneva Learning Foundation’s Accelerator, every participant commits to work toward their countries’ goals, and to do so by using the best available global knowledge.
Learn more: What is The Geneva Learning Foundation’s Impact Accelerator?
This actually supports effective adoption and use of global guidelines, which otherwise may linger on shelves.
In fact, we have shown in the past that this mechanism increases adherence to proven protocols (e.g., WHO guidelines on heat stress or malaria control). That is one important reason why it is a powerful implementation science tool. It transforms adherence from a wish expressed in the capital city into a reality in local communities.
Furthermore, if national planners and international experts are willing to listen, they may hear back ways to improve and strengthen the global standards, as well as gain new insights into the “how” of local implementation that defies easy generalization.
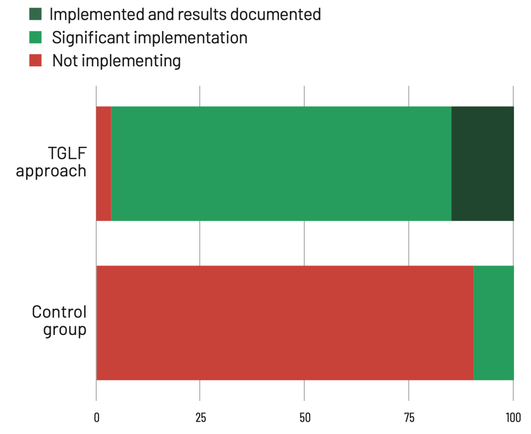
When we compared this model to conventional technical assistance or “cascade training,” the results were stark :
These results give us confidence. We are not starting from zero. We are building on prior work in immunization and other areas of work where supporting implementation led to exactly these kinds of validated outcomes.
Here are two examples of local solutions in action.
- Côte d’Ivoire: Communities identified stagnant water as a malaria risk and organized youth-led cleanup committees to clear gutters. This resulted in a drastic, locally measured drop in malaria cases.
- Cameroon: In response to frequent floods, communities voluntarily cleaned gutters to ensure water did not stagnate, directly impacting disease vectors.
No one in the capital city – and certainly no one in Geneva or Seattle – knew about these initiatives.
This leads to our most ambitious projection. If we can grow this network from 80,000 to 1 million health workers by 2030, we estimate we could save 7 million lives through simple, locally resourced projects, at a cost of less than $2 per life.
I acknowledge this is an aggressive claim. It is a “back-of-the-envelope” calculation based on our pilot data. It assumes that local projects remain effective at scale and that we can attribute outcomes to the network. But I ask you: if there is even a glimmer of a chance that this is true – that we can save lives at a fraction of the cost of traditional interventions – isn’t it worth investing in the rigorous research to find out?
Discussion
Do you think MOOCs (Massive Open Online Courses) are dead?
Reda Sadki: MOOCs have become primarily marketing tools for higher education. From a pedagogical perspective, they remain transmissive, expert to learner. I do not see how that model can deliver against complex problems. We need a two-way street. We need new ways to organize the production and circulation of knowledge.
Thank you, Reda. I noticed in your results that food security is a major concern. Have you identified local actions focusing on food, given the challenges of working with healthcare workers who might not see this as their primary remit?
Reda Sadki: That is a critical question. Food insecurity is one of the most worrying consequences we are tracking. We often see a mismatch where local actors tasked with, say, immunization, do not see nutrition as their lane. However, at the community level, the approach is naturally integrated – the health worker knows the vet, who knows the farmers. Those connections exist.
We are currently preparing a major insights report that includes a specific chapter on food security. We are also designing an accelerator specifically around this topic to bring together the right set of partners, because the consequences we are documenting are dire.
You mentioned that 78% of participants eventually said “no thank you” to further support. Ideally, shouldn’t these peer networks become self-sustaining, bypassing Geneva or London entirely?
Reda Sadki: That is the goal. We have shown that more than half of each cohort stays in touch to continue leading local action. However, as long as resources and decision-making power remain concentrated in global centers, we cannot just “flip a switch”. We need to build bridges that facilitate that transformation. The goal is autonomy, but the reality requires us to actively dismantle the dependencies that current funding structures create.
Are there new capabilities that we in academia need to develop urgently to support this?
Reda Sadki: It is about moving away from being the “sage on the stage” to a “guide on the side”. For example, in our recent work, global partners and experts joined Teach to Reach sessions not to present the latest guidelines, but to listen to the challenges local practitioners faced. They then had to figure out how their expertise could be useful in response to those specific needs.
For researchers inside academic institutions, this can be difficult. It requires starting not with a research question, but with a willingness to listen to the needs of local actors and let the research questions emerge from that reality. We know this challenges the incentive structures of academia, but we are open to partnering with researchers willing to work in this emergent, demand-driven way.
It is a fascinating dilemma – we want to be guided by needs, but funding requires pre-set hypotheses. Reda, this has been truly impressive. Thank you for sharing these refreshing perspectives.
Reda Sadki: Thank you. We look forward to exploring how we can collaborate. Best wishes for the holidays and the new year.
References
Images: The Geneva Learning Foundation Collection © 2025
#CharlotteMbuh #climateAndHealth #epistemology #globalHealth #ImpactAccelerator #implementationResearch #LSHTM #MassiveOpenOnlineCourses #PaulinePaterson #peerLearning #TeachToReach #TheGenevaLearningFoundation