This #LungCancerAwarenessMonth, we honor those we've lost and fight for a brighter future.
Learn more about lung cancer and empower yourself to take action. Please register for our FREE live OncTalk on December 14 at 11:00 AM ET.
Click here to register: https://give.cancergrace.org/event/lung-cancer-onctalk-december-2024/e630685
Knowledge is power!
Let's spread awareness and hope together. #LCSM #CancerSupport #LungCancerWebinar #LungCancer
Lung Cancer ONCTalk December 2024
{{MetaTags.description}}
#FlashbackFriday to this article we posted earlier this year in honor of 🫁 #LungCancerAwarenessMonth!
Click the link below to have a look 👇
----------------------------------------------
Evaluating whether changes in attenuation of the 🫁 #lung parenchyma adjacent to a nodule affect the performance of #nodule segmentation using CT studies and volumetric tools. (Diana Penha et al.)
#InsightsIntoImaging
🔗 https://insightsimaging.springeropen.com/articles/10.1186/s13244-021-01027-0/figures/2
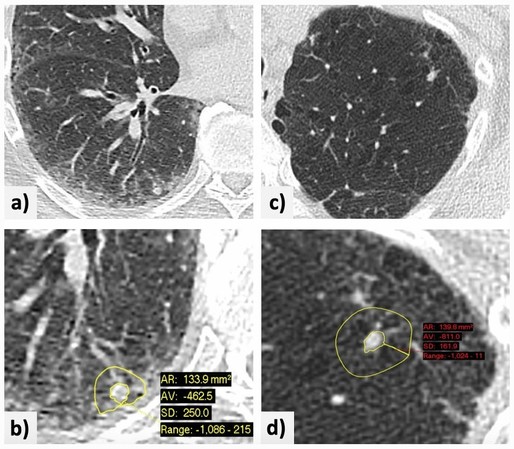

The impact of lung parenchyma attenuation on nodule volumetry in lung cancer screening - Insights into Imaging
Background Recent recommendations for lung nodule management include volumetric analysis using tools that present intrinsic measurement variability, with possible impacts on clinical decisions and patient safety. This study was conducted to evaluate whether changes in the attenuation of the lung parenchyma adjacent to a nodule affect the performance of nodule segmentation using computed tomography (CT) studies and volumetric tools. Methods Two radiologists retrospectively applied two commercially available volumetric tools for the assessment of lung nodules with diameters of 5–8 mm detected by low-dose chest CT during a lung cancer screening program. The radiologists recorded the success and adequacy of nodule segmentation, nodule volume, manually and automatically (or semi-automatically) obtained long- and short-axis measurements, mean attenuation of adjacent lung parenchyma, and presence of interstitial lung abnormalities or disease, emphysema, pleural plaques, and linear atelectasis. Regression analysis was performed to identify predictors of good nodule segmentation using the volumetric tools. Interobserver and intersoftware agreement on good nodule segmentation was assessed using the intraclass correlation coefficient. Results In total, data on 1265 nodules (mean patient age, 68.3 ± 5.1 years; 70.2% male) were included in the study. In the regression model, attenuation of the adjacent lung parenchyma was highly significant (odds ratio 0.987, p < 0.001), with a large effect size. Interobserver and intersoftware agreement on good segmentation was good, although one software package performed better and measurements differed consistently between software packages. Conclusion For lung nodules with diameters of 5–8 mm, the likelihood of good segmentation declines with increasing attenuation of the adjacent parenchyma.
Study shows results of HUNCHEST-II, the largest population-based LDCT screening program in #Hungary, including the characteristics of the #LungCancer cases. (Anna Kerpel-Fronius et al.)
#EuropeanRadiology #LungCancerAwarenessMonth
🔗 https://link.springer.com/article/10.1007/s00330-023-10379-8

HUNCHEST-II contributes to a shift to earlier-stage lung cancer detection: final results of a nationwide screening program - European Radiology
Objectives The introduction of low-dose CT (LDCT) altered the landscape of lung cancer (LC) screening and contributed to the reduction of mortality rates worldwide. Here we report the final results of HUNCHEST-II, the largest population-based LDCT screening program in Hungary, including the screening and diagnostic outcomes, and the characteristics of the LC cases. Methods A total of 4215 high-risk individuals aged between 50 and 75 years with a smoking history of at least 25 pack-years were assigned to undergo LDCT screening. Screening outcomes were determined based on the volume, growth, and volume doubling time of pulmonary nodules or masses. The clinical stage distribution of screen-detected cancers was compared with two independent practice-based databases consisting of unscreened LC patients. Results The percentage of negative and indeterminate tests at baseline were 74.2% and 21.7%, respectively, whereas the prevalence of positive LDCT results was 4.1%. Overall, 76 LC patients were diagnosed throughout the screening rounds (1.8% of total participants), out of which 62 (1.5%) patients were already identified in the first screening round. The overall positive predictive value of a positive test was 58%. Most screen-detected malignancies were stage I LCs (60.7%), and only 16.4% of all cases could be classified as stage IV disease. The percentage of early-stage malignancies was significantly higher among HUNCHEST-II screen-detected individuals than among the LC patients in the National Koranyi Institute of Pulmonology’s archive or the Hungarian Cancer Registry (p < 0.001). Conclusions HUNCHEST-II demonstrates that LDCT screening for LC facilitates early diagnosis, thus arguing in favor of introducing systematic LC screening in Hungary. Clinical relevance statement HUNCHEST-II is the so-far largest population-based low-dose CT screening program in Hungary. A positive test’s overall positive predictive value was 58%, and most screen-detected malignancies were early-stage lesions. These results pave the way for expansive systematic screening in the region. Key Points • Conducted in 18 medical facilities, HUNCHEST-II is the so far largest population-based low-dose CT screening program in Hungary. • The vast majority of screen-detected malignancies were early-stage lung cancers, and the overall positive predictive value of a positive test was 58%. • HUNCHEST-II facilitates early diagnosis, thus arguing in favor of introducing systematic lung cancer screening in Hungary.
📢 Let’s continue #LungCancerAwarenessMonth & join #TumorBoardTuesday!!
🥼@Latinamd @SamuelKareffMD bring us through treating #NSCLC with neoadju IO
Join us here!👇🏽
📱Weigh in how YOU’D treat
🧾Bring receipts
🙋Ask Q’s
📊check polls
🔁RT
👩🏻⚕️tag peers
@MPishvaian @JohnEbbenMDPhD
---
RT @SamuelKareffMD
@TumorBoardTues 1/16 #TumorBoardTuesday #LungCancer #OncTwitter
69yo 👩🏻🦱
9 pk/yr tobacco - quit 34 years ago
3-4 months of cough & spu…
https://twitter.com/SamuelKareffMD/status/1592683889210032129
Samuel Kareff, MD, MPH on Twitter
“@TumorBoardTues 1/16 #TumorBoardTuesday #LungCancer #OncTwitter
69yo 👩🏻🦱
9 pk/yr tobacco - quit 34 years ago
3-4 months of cough & sputum
🩻CT: 5.6-cm RLL hypermetabolic mass
🧲MRI: brain negative
EBUS➡️ ipsilateral hilar lymphadenopathy (#10R)
🔬adenocarcinoma of 🫁
StageIIIA (cT3N1M0) #NSCLC”
#TumorBoardTuesday #LungCancerAwarenessMonth
🙌Immunotherapy has been transformational for advanced #lungcancer
📢Join us tomorrow, Tuesday 11.15.22 at 8pm ET as @Latinamd & @SamuelKareffMD 🧑🏫us on the💥of immunotherapy in the neoadjuvant space for #NSCLC‼️
#TumorBoardTuesday #LungCancerAwarenessMonth
@Latinamd @SamuelKareffMD
📅Tues, 11/15/22 8PM ET
✅polls
⚖️in & bring citations🧾
🔁Retweet & tag your colleagues
🏆Earn your🆓CME (AMA & MOC) http://integrityce.com/tbt
Before the case:🧐tell us where you are in your 🩺journey👇👇👇
Page not found - Integrity CE