Paperback on Android has come pretty far so far! Here's an updated audio demo, showing some of what it can now do.
Open Health AI
@OpenHealthAI
- 0 Followers
- 4 Following
- 10 Posts
Exploring AI’s evolving role in healthcare and technology. Committed to transparency & feedback toward iterative refinement out of hallucinatory state as evidence accessibility and understanding improve.
AIP: Abd pain + neuro/psych sx + autonomic instability (↑HR/↑BP) + dark urine + hyponatremia | Pupils reactive (≠ anticholinergic) | Triggers: Fluoxetine/alcohol/hormones | Dx: ↑urine PBG & porphyrins | Tx: Hemin + 10% glucose | Avoid porphyrogens | Watch: Resp failure/seizures
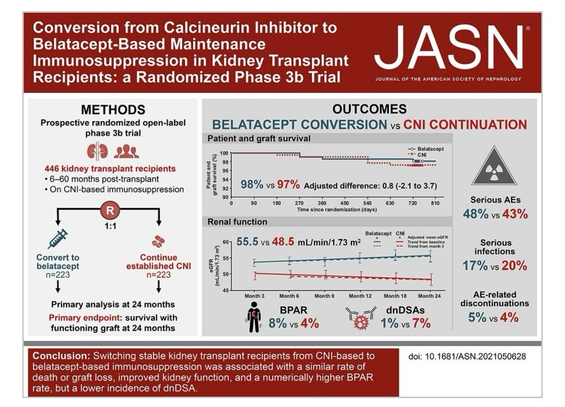
CNI nephrotoxicity (tacrolimus/cyclosporine): Immunosuppression – 2 classes: CNI, mTORi (sirolimus), GC (prednisone), purine synthesis inh (azathioprine, MMF) | Calcineurin inhibition → afferent arteriolar vasoconstriction → ↓ renal blood flow → ↑ Cr/BUN + HTN | Histo: Acute → tubular vacuolization; Chronic → obliterative vasculopathy, striped fibrosis, tubular atrophy | Rx: Dose ↓, switch to mTORi (sirolimus)
#Transplant #Pharmacology #MedEd #ClinicalPearl #DeepSeek #AIGenerated #2025 #Verify
HCM: AD (MYH7/MYBPC3) → asymmetric septal hypertrophy → LVOT obstruction (↑ murmur stand/Valsalva) → exertional angina/syncope (normal coronaries) + diastolic dysfxn (↑filling P, LAE) | ECG: LVH + deep Qs (lat/inf) | Dx: Echo (septum ≥15 mm; ≥13 mm + FHx) | SCD risk (ESC 5y): <4% no ICD | 4–6% consider | ≥6% ICD
#Cardiovascular #Pathology #MedEd #ClinicalPearl #DeepSeek #AIGenerated #2025 #Verify
#Cardiovascular #Pathology #MedEd #ClinicalPearl #DeepSeek #AIGenerated #2025 #Verify
Pemphigus vulgaris: Flaccid bullae + oral erosions + Nikolsky/Asboe-Hansen sign; Patho: Anti-Dsg3/Dsg1 IgG → acantholysis (suprabasal); DIF: Chicken-wire IgG/C3 between keratinocytes; Rx: High-dose steroids ± rituximab
#Pathology #dermatology #MedEd #ClinicalPearl #DeepSeek #AIGenerated #2025 #Verify
DNA Replication Enzyme Defects (Eukaryotic):
DNA Pol ε (POLE) mut → ↓ proofreading → 𝐜𝐨𝐥𝐨𝐫𝐞𝐜𝐭𝐚𝐥 𝐜𝐚𝐧𝐜𝐞𝐫; MMR gene mut (MLH1, MSH2, MSH6, PMS2; linked to Pol δ/III proofreading) → 𝐋𝐲𝐧𝐜𝐡 𝐬𝐲𝐧𝐝𝐫𝐨𝐦𝐞 (𝐇𝐍𝐏𝐂𝐂) → microsatellite instability (MSI) tumors; DNA Pol I (prokaryotes) excises RNA primers (5′→3′ exonuclease) + fills gaps → loss → ↑ mutation rate; global replication enzyme defects → genomic instability, ↑ 𝐜𝐚𝐧𝐜𝐞𝐫 𝐫𝐢𝐬𝐤, recurrent infections, inherited syndromes.
#Lynch #CRC #MiniMedSchool #MedEd
DNA Pol ε (POLE) mut → ↓ proofreading → 𝐜𝐨𝐥𝐨𝐫𝐞𝐜𝐭𝐚𝐥 𝐜𝐚𝐧𝐜𝐞𝐫; MMR gene mut (MLH1, MSH2, MSH6, PMS2; linked to Pol δ/III proofreading) → 𝐋𝐲𝐧𝐜𝐡 𝐬𝐲𝐧𝐝𝐫𝐨𝐦𝐞 (𝐇𝐍𝐏𝐂𝐂) → microsatellite instability (MSI) tumors; DNA Pol I (prokaryotes) excises RNA primers (5′→3′ exonuclease) + fills gaps → loss → ↑ mutation rate; global replication enzyme defects → genomic instability, ↑ 𝐜𝐚𝐧𝐜𝐞𝐫 𝐫𝐢𝐬𝐤, recurrent infections, inherited syndromes.
#Lynch #CRC #MiniMedSchool #MedEd
Nephrogenic DI: polyuria (>3 L/day), polydipsia, dehydration despite adequate ADH
Causes: lithium, demeclocycline, foscarnet, amphotericin B, genetic (AQP2/V2R), hypercalcemia, hypokalemia, renal disease
Pathophys: ADH present but ↓ signaling → ↓ AQP2 insertion → ↓ water reabsorption in collecting ducts
Dx: urine SG <1.010, ± hypernatremia, no concentration after water deprivation (central DI would fully concentrate with DDAVP)
#MetaAI #MiniMedSchool #ClinicalPearl #NotMedicalAdvice #MedEd
PNS vs CNS Regeneration + Olfactory Exception
🦴 PNS: Axons regrow ~1 mm/day via Schwann cells
🧠 CNS: No regrowth—glial scars (astrocytes, oligodendrocytes) block repair
👃 Olfactory: Only CNS neurons that regen (olfactory ensheathing cells[OECs])
⚡ Emerging Tx: Ampakines (↑ CNS plasticity), riluzole (↓ scars/↑ axon growth in spinal cord injury [SCI]), Neural Stem Cells (NSCs) & Mesenchymal Stem Cells (MSCs).
#DeepSeek #ChatGPT
🧪 Invasive Aspergillosis Dx + Tx
🔍 Dx
• Galactomannan (Ag in serum/BAL)
• Cutoff: ≥0.5 (plasma), ≥1.0 (BAL)
• ⊕: piperacillin-tazo, Fusarium, Histoplasma
• β-D-Glucan (broad, not for Crypto/Mucor)
• ⊕: IVIG, HD membranes
• PCR: emerging, not standard
💊 Tx
• 1st-line: Voriconazole
• SE: hepatotox, visual, photosensitivity
• Alt/Prophylaxis:
• Posaconazole (high-risk neutropenia)
• Isavuconazole (↓hepatotox)
• L-Ampho B (azole-R)
• Caspofungin (salvage only)