#Singapore, New weekly #COVID19 cases admitted to #hospitals and #ICUs highest for 2023 https://www.channelnewsasia.com/singapore/covid19-weekly-cases-hospital-icu-highest-2023-4005086

''6 Oct. '23 Highlights: * during surveillance week, the incidence of new detected cases of #COVID19 remained low and overall stable. * #Impact on #healthcare system, especially #ICUs was limited. * Predominance of #omicron #XBB lineages was confirmed, especially with #EG5 subvariant, similarly other European regions.'' #surveillance #italy #SARS_COV_2
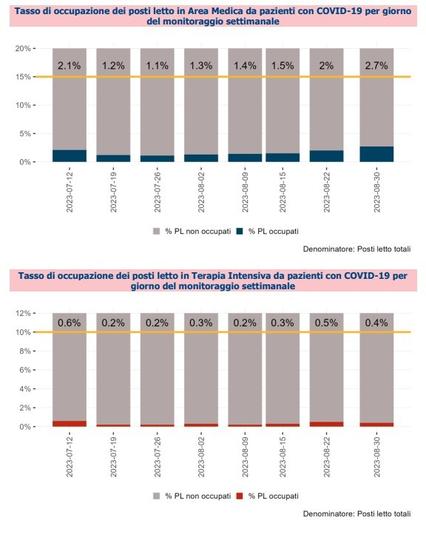
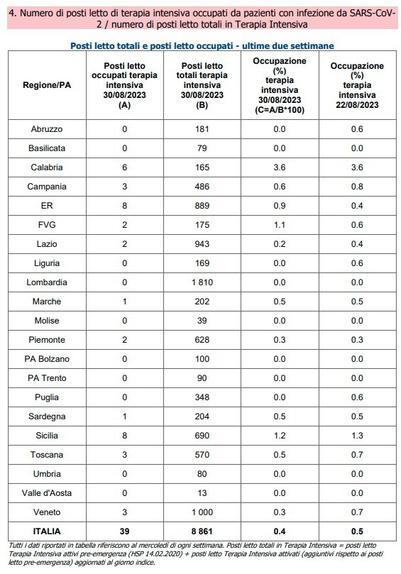
''Cases' incidence is now 52 per 100,000, compared to 36 of last week. #ICUs beds occupancy has risen too. Call to vaccinate the most at risk.''
#COVID19-associated #pulmonary #aspergillosis in mechanically ventilated patients: a prospective, multicentre #UK study, Thorax: https://thorax.bmj.com/content/early/2023/09/01/thorax-2023-220002 #research #medicine #SARS_CoV_2 #ICUs

COVID-19-associated pulmonary aspergillosis in mechanically ventilated patients: a prospective, multicentre UK study
Background Invasive pulmonary aspergillosis is a complication of severe COVID-19, with regional variation in reported incidence and mortality. We describe the incidence, risk factors and mortality associated with COVID-19-associated pulmonary aspergillosis (CAPA) in a prospective, multicentre UK cohort. Methods From March 2020 to March 2021, 266 mechanically ventilated adults with COVID-19 were enrolled across 5 UK hospital intensive care units (ICUs). CAPA was defined using European Confederation for Medical Mycology and the International Society for Human and Animal Mycology criteria and fungal diagnostics performed on respiratory and serum samples. Results Twenty-nine of 266 patients (10.9%) had probable CAPA, 14 (5.2%) possible CAPA and none proven CAPA. Probable CAPA was diagnosed a median of 9 (IQR 7–16) days after ICU admission. Factors associated with probable CAPA after multivariable logistic regression were cumulative steroid dose given within 28 days prior to ICU admission (adjusted OR (aOR) 1.16; 95% CI 1.01 to 1.43 per 100 mg prednisolone-equivalent), receipt of an interleukin (IL)-6 inhibitor (aOR 2.79; 95% CI 1.22 to 6.48) and chronic obstructive pulmonary disease (COPD) (aOR 4.78; 95% CI 1.13 to 18.13). Mortality in patients with probable CAPA was 55%, vs 46% in those without. After adjustment for immortal time bias, CAPA was associated with an increased risk of 90-day mortality (HR 1.85; 95% CI 1.07 to 3.19); however, this association did not remain statistically significant after further adjustment for confounders (adjusted HR 1.57; 95% CI 0.88 to 2.80). There was no difference in mortality between patients with CAPA prescribed antifungals (9 of 17; 53%) and those who were not (7 of 12; 58%) (p=0.77). Interpretation In this first prospective UK study, probable CAPA was associated with corticosteroid use, receipt of IL-6 inhibitors and pre-existing COPD. CAPA did not impact mortality following adjustment for prognostic variables. Data are available upon reasonable request. All de-identified, individual participant data that underlie the reported results of this article, as well as the data dictionary, study material (protocols, consent forms, patient information sheets) and the R analytical code, are available from the corresponding author on reasonable request.
{Trends in occupation rate of acute beds and #ICUs} {Yellow line is the emergency threshold}

#Russia, A reserve of #beds for #patients with signs of {#cider} #poisoning has been created in the #ICUs of the #Ulyanovsk region - Читайте на WWW.UL.KP.RU: https://www.ul.kp.ru/online/news/5302489/
#SpaceSaturday: A United Launch Alliance Delta IV Heavy #rocket #launched #NASA’s #Orion #spacecraft on Exploration Flight Test 1, or #EFT1.
The Delta IV Heavy was chosen as the post powerful and compatible rocket for the Orion test capsule, since its upper stage, the Delta Cryogenic Second Stage, serves as the basis for the Interim Cryogenic Upper Stage on the #SLS #rocket.
The #Delta4 could lift the capsule into a trajectory that would cause it to re-enter the atmosphere at similar velocities as a lunar return, proving the heat shield, parachutes, and landing systems.
It also verified the #LaunchAbortSystem disposal and fairing jettison.
#Delta4, #Delta4Heavy, #ExplorationFlightTest1, #RocketLaunch, #DeltaCryogenicSecondStage, #DCSS, #InterimCryogenicUpperStage, #ICUS, #UnitedLaunchAlliance, #ULA
https://heronfox.pixels.com/featured/delta-iv-with-orion-climbs-heron-and-fox.html
The Delta IV Heavy was chosen as the post powerful and compatible rocket for the Orion test capsule, since its upper stage, the Delta Cryogenic Second Stage, serves as the basis for the Interim Cryogenic Upper Stage on the #SLS #rocket.
The #Delta4 could lift the capsule into a trajectory that would cause it to re-enter the atmosphere at similar velocities as a lunar return, proving the heat shield, parachutes, and landing systems.
It also verified the #LaunchAbortSystem disposal and fairing jettison.
#Delta4, #Delta4Heavy, #ExplorationFlightTest1, #RocketLaunch, #DeltaCryogenicSecondStage, #DCSS, #InterimCryogenicUpperStage, #ICUS, #UnitedLaunchAlliance, #ULA
https://heronfox.pixels.com/featured/delta-iv-with-orion-climbs-heron-and-fox.html

