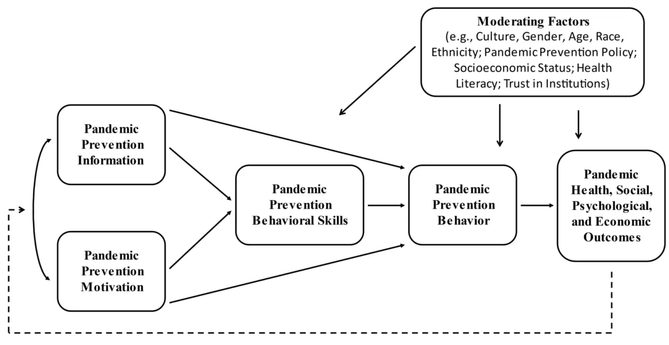
🚨PublicationAlert! Jeffrey & William Fisher unveil their IMB Model of Pandemic Risk & Prevention in
http://advances.in psychology.
#COVID19 won't be our last pandemic, their model equips us to foster the behavior change crucial for future outbreaks.
https://advances.in/psychology/10.56296/aip00004/
Advances.in - Reinventing Academic Publishing
Traditional publishers take advantage of free labor by overburdened academics. Advances.in aims to change this by paying editors and reviewers for their work.
🚨New study with an animal model shows that the senolytics dasatinib and quercetin (D/Q) significantly reduced SARS-CoV-2-related mortality, delayed its onset, and reduced the number of other clinical symptoms. Could it reduce risks of
#LongCovid?
https://onlinelibrary.wiley.com/doi/10.1111/acel.13771🚨 Symptoms of
#LongCovid and
#MECFS overlapped almost perfectly in a study (average correlation of .9). Like LC, MECFS most often starts after an infection. Although some don't like to hear it, evidence is growing that both represent the same condition.
https://www.mdpi.com/2227-9059/11/1/180

Converging Evidence of Similar Symptomatology of ME/CFS and PASC Indicating Multisystemic Dyshomeostasis
The purpose of this article is to review the evidence of similar symptomatology of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and post-acute sequelae of SARS-CoV-2 infection (PASC). Reanalysis of data from a study by Jason comparing symptom reports from two groups of ME/CFS and PASC patients shows a notably similar symptomatology. Symptom scores of the PASC group and the ME/CFS group correlated 0.902 (p < 0.0001) across items. The hypothesis is presented that ME/CFS and PASC are caused by a chronic state of multisystemic disequilibrium including endocrinological, immunological, and/or metabolic changes. The hypothesis holds that a changed set point persistently pushes the organism towards a pathological dysfunctional state which fails to reset. To use an analogy of a thermostat, if the ‘off switch’ of a thermostat intermittently stops working, for periods the house would become warmer and warmer without limit. The hypothesis draws on recent investigations of the Central Homeostasis Network showing multiple interconnections between the autonomic system, central nervous system, and brain stem. The hypothesis helps to explain the shared symptomatology of ME/CFS and PASC and the unpredictable, intermittent, and fluctuating pattern of symptoms of ME/CFS and PASC. The current theoretical approach remains speculative and requires in-depth investigation before any definite conclusions can be drawn.
🚨New study finds that high peak body temp and low oxygen saturation during acute COVID can lead to long-term physical and mental health issues, because they contribute to neurotoxicity caused by immune and oxidative stress in
#LongCovid.
https://www.mdpi.com/2077-0383/12/2/511

Chronic Fatigue, Depression and Anxiety Symptoms in Long COVID Are Strongly Predicted by Neuroimmune and Neuro-Oxidative Pathways Which Are Caused by the Inflammation during Acute Infection
Background: Long-term coronavirus disease 2019 (long COVID) is associated with physio-somatic (chronic fatigue syndrome and somatic symptoms) and affective (depression and anxiety) symptoms. The severity of the long COVID physio-affective phenome is largely predicted by increased peak body temperature (BT) and lowered oxygen saturation (SpO2) during the acute infectious phase. This study aims to delineate whether the association of BT and SpO2 during the acute phase and the long COVID physio-affective phenome is mediated by neurotoxicity (NT) resulting from activated immune-inflammatory and oxidative stress pathways. Methods: We recruited 86 patients with long COVID (3–4 months after the acute phase) and 39 healthy controls and assessed serum C-reactive protein (CRP), caspase 1, interleukin (IL) 1β, IL-18, IL-10, myeloperoxidase (MPO), advanced oxidation protein products (AOPPs), total antioxidant capacity (TAC), and calcium (Ca), as well as peak BT and SpO2 during the acute phase. Results: Cluster analysis revealed that a significant part (34.9%) of long COVID patients (n = 30) show a highly elevated NT index as computed based on IL-1β, IL-18, caspase 1, CRP, MPO, and AOPPs. Partial least squares analysis showed that 61.6% of the variance in the physio-affective phenome of long COVID could be explained by the NT index, lowered Ca, and peak BT/SpO2 in the acute phase and prior vaccinations with AstraZeneca or Pfizer. The most important predictors of the physio-affective phenome are Ca, CRP, IL-1β, AOPPs, and MPO. Conclusion: The infection–immune–inflammatory core of acute COVID-19 strongly predicts the development of physio-affective symptoms 3–4 months later, and these effects are partly mediated by neuro-immune and neuro-oxidative pathways.
🚨 The number of people waiting for hospital treatment in the UK has nearly doubled since the pandemic began among some medical specialties. Likely the same many other places.
https://www.dailymail.co.uk/health/article-11508743/The-NHS-waiting-lists-hit-HARDEST-Covid.html
The NHS waiting lists hit HARDEST by Covid
The NHS England backlog hit a 7.2million in October - the highest figure since records began 15 years ago and two-thirds more than the number logged in March 2020.
🚨 In a large-scale meta-analysis with more than 20 million participants, "COVID-19 survivors had an additional 90% risk of developing incident heart failure after COVID-19 infection in the long-term period."
#LongCovid https://pubmed.ncbi.nlm.nih.gov/36572763/
Risk of incident heart failure after COVID-19 recovery: a systematic review and meta-analysis - PubMed
Patients recovered from COVID-19 have an increased incidence of cardiovascular disease and heart structural changes. The aim of the present manuscript is to assess the risk of incident heart failure (HF) after COVID-19 infection. Data were obtained searching MEDLINE and Scopus for all studies publis …
🚨 A common misconception is that we do not need to focus on
#LongCovid because most people get well over time. Turns out that this is not true. A new meta-analysis shows that symptoms on average decrease by 50% during the first month but then stabilize.
https://www.valueinhealthjournal.com/article/S1098-3015(22)04743-X/fulltext🚨"Across 66 countries (N = 46,450), people living in countries with higher conflict intensity tended to be more susceptible to COVID-19 conspiracy beliefs."
https://psycnet.apa.org/record/2023-13860-001Compared to the control group, treatment with nirmatrelvir (Paxlovid) was associated with reduced risk of
#LongCovid including a large range of symptoms.
https://www.medrxiv.org/content/10.1101/2022.11.03.22281783v1.full.pdf