Reading a recent paper covering PSA testing for transfeminine people (doi:10.1001/jama.2024.9997). One small thing bothers me is this kind of language; if not for it feeling a little inappropriate, the paper doesn't separate androgenic suppression from estrogen levels.
#transhealth
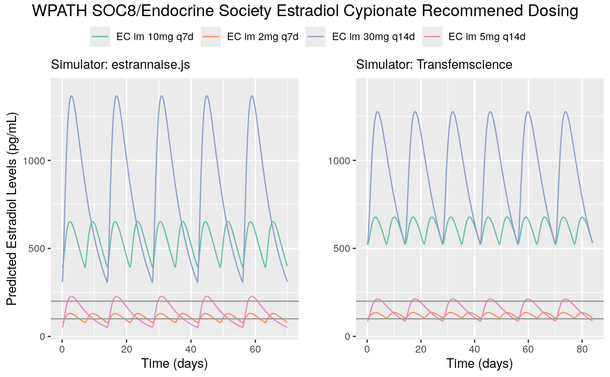
This is still profound but not as extreme with Estradiol cypionate. Comparing between the models we observe some variation in the scaling, however the overall "shape" appears the same with both showing dosing that appears considerably out of range.
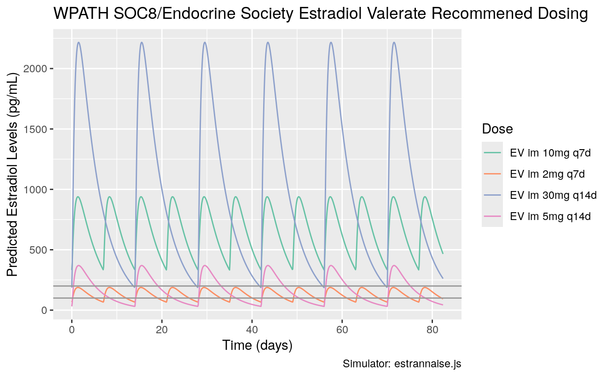
If we take the existing known models of how these esters perform, for the advised dosing ranges, levels are projected to either be considerably high at peak, or fall below. For Estradiol valerate, there is a notable contrast between the lower end of dosing and the higher end.
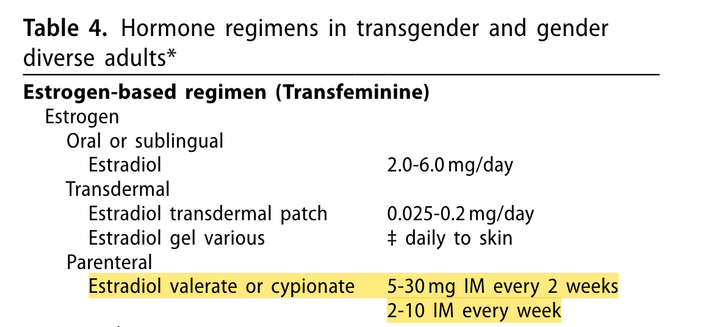
WPATH and Endocrine Society currently advise a single range of dosing for both Estradiol valerate and Estradiol cypionate, starting at 2mg weekly, up to a maximum dose of 30mg every fortnight. These two esters have different behaviours in terms of serum Estradiol levels, with Estradiol cypionate having high fat solubility and subsequently slower rate of release from the depot.
Currently WPATH SOC8 aligns itself with the Endocrine Society in terms of both dosing recommendations and target hormonal levels patients should be achieving, which is 100-200 pg/mL (~370-750 pmol/L). It's important to note this is an expected average level, and that throughout the dosing cycle it can go above or below that mark.
Impact of cancer risks are admittedly complicated due to many variables. The section of HRT use in breast cancer survivors is confusing, on one part hand waves "generally not advised" then proceeds to describe how several meta-analyses found a reduction of reoccurrence. I'm worried this phrasing may confuse providers, or encourage negative behaviours.
Guidance also suggests the use of oral progesterone in patients affected by sleeping disturbances, noting the "possibility" of GABA-agonstic effect. Oral administration doesn't produce meaningful P4 levels - Levine & Watson, 2000 (doi:10.1016/S0015-0282(99)00553-1) observed for 100mg po qd a max/avg of 2ng/mL and 0.14ng/mL, far lower than mean pre-menopausal levels and likely ineffective at providing hormonal benefit to the body. More bluntly - it's just sedating patients.
NAMS's 2022 menopausal HRT statement (doi:10.1097/GME.0000000000002028) has an entire section attempting to dissuade care providers from prescribing compounded HRT. In it, it suggests that dosing based on serum results may be unreliable. This misses nuance - it's only less accurate if timing of dose and the context of ROA are not taken into consideration. In trans healthcare, we do this by measuring serum levels either at midpoint or trough in cycle.