🧵 Dosing recommendations for injectable forms of Estradiol don't seem to line up with the recommended serum hormone ranges, are likely making it harder for providers and patients to achieve ideal hormonal levels, and are likely impacting quality of life. Let's look at what might be going on.
Dosing recommendations for providers comes in multiple places: international standards of care guidance, regional guidance, and practice information. There's also some guidance that happens as a result of "process pollination" from practitioners and their management choosing to adopt various guides. What providers actually prescribe patients comes down to not only the guidance, but also regional drug availability, their experience, and to a lesser extent patient preference/experiences.
Injectable feminising HRT in the global north is largely limited to the USA, parts of Eastern Europe, and Japan. There are exceptions; both Canada and Australia have a very small number of practitioners prescribing, but in both circumstances it's considered much more "off label" and is much more expensive due to insurance. In western Europe it's mostly non-existent, and there seems to be a weird correlation between how regulated/capitalist a given medical system is to it's availability.
When writing guidance on dosing there's a few factors that have to be taken into considering: medication packaging and how doses are dispensed to patients, ease of communication and administration to the patient so they can be consistent in dosing (particularly if they are self-administering), as well as the general rule of titration - use the least amount that's most effective.
Currently WPATH SOC8 aligns itself with the Endocrine Society in terms of both dosing recommendations and target hormonal levels patients should be achieving, which is 100-200 pg/mL (~370-750 pmol/L). It's important to note this is an expected average level, and that throughout the dosing cycle it can go above or below that mark.

With mean levels below that mark patients are at risk of being unable to suppress endogenous production if doing monotherapy or intermittent hormonal starvation, with levels being higher at greater risk of thrombotic events. Higher variation in peak to mean in levels during the dosing cycle can see changes in mood and feelings, particularly towards end of cycle, impacting quality of life.
WPATH and Endocrine Society currently advise a single range of dosing for both Estradiol valerate and Estradiol cypionate, starting at 2mg weekly, up to a maximum dose of 30mg every fortnight. These two esters have different behaviours in terms of serum Estradiol levels, with Estradiol cypionate having high fat solubility and subsequently slower rate of release from the depot.
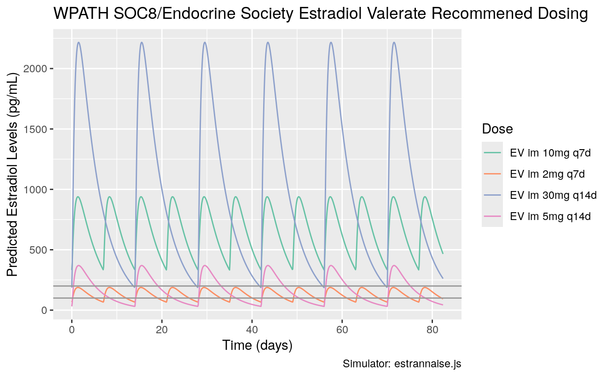
ℹ️ A quick word to interpreting the following graphs: these are created from the data used in two simulators, which in turn are modelled based on various research which collected serum Estradiol levels. What patients achieve on dosing will vary considerably based on a multitude of factors, however we can infer common trends from them. In all diagrams there are two lines marked at 100 pg/mL and 200 pg/mL to mark where average levels where the provider guidance advises.
If we take the existing known models of how these esters perform, for the advised dosing ranges, levels are projected to either be considerably high at peak, or fall below. For Estradiol valerate, there is a notable contrast between the lower end of dosing and the higher end.
This is still profound but not as extreme with Estradiol cypionate. Comparing between the models we observe some variation in the scaling, however the overall "shape" appears the same with both showing dosing that appears considerably out of range.
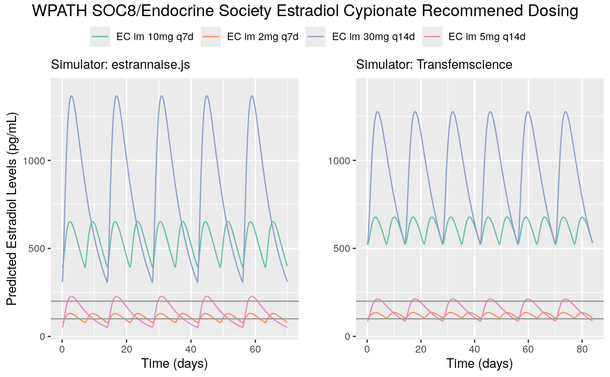
These ranges are unlikely to have patients within the target ranges throughout the dosing cycle, which may be resulting in some providers not prescribing effective or safer dosing. With such variance in peak and trough, patients will be at noted risk not only to thrombotic events as these correlate to higher levels, but also may be struggling with endogenous suppression as well as rapid mood shifts, particularly towards the end of the cycle in the day or two leading up to the next schedule dose.
What might more appropriate dosing ranges look like? Instead of communicating only a potential range, it would likely be better advising starting doses and then advise maximum dosing - with several starting doses advised so patients have options to fit within lifestyle leading to consistency in dosing. Such guidance should also handle patients who don't require larger dosing as part of monotherapy either because they are using an antigondatropic (e.g. a GnRHa) or have had a gonadectomy.
Different esters should also have different dosing recommendations where the release profile varies, this is what other guidance (e.g. Fenway) advises. There also seems to be a push towards shortest interval of weekly - although for many it's desirable to inject as infrequently as possible, this does not lend itself well to the pharmacokinetic behaviours of the available esters and that if looking at shorter intervals of every five days or twice weekly administration may be better options.