Science for ME: News in Brief
23 - 29 Mar 2026
🧵 of highlighted #MECFS and #LongCovid research papers being discussed this week on the Science for ME forum.
@mecfs
https://www.s4me.info/threads/news-in-brief-march-2026.49238/post-683994
Science for ME: News in Brief
23 - 29 Mar 2026
🧵 of highlighted #MECFS and #LongCovid research papers being discussed this week on the Science for ME forum.
@mecfs
https://www.s4me.info/threads/news-in-brief-march-2026.49238/post-683994
Expert perspectives on Myalgic encephalomyelitis/chronic fatigue syndrome – Insights from the 3rd International Conference of the Charité Fatigue Center — Fehrer et al
"the conference provided a comprehensive overview of state-of-the-art research on ME/CFS, covering recent advances in patient care and mechanistic insights into cardiovascular dysregulation, metabolic dysfunction, and immune dysregulation."
https://www.sciencedirect.com/science/article/pii/S1568997226000571
Commentary: Cognitive behavioural therapy for the treatment of chronic fatigue syndrome in adults: a short analysis of the meta-analysis — Vink and Vink-Niese
"In conclusion, our analysis confirms the conclusion by NICE that the quality of CBT studies is (very) low and that CBT, irrespective of the form that is used, is not an effective treatment for ME/CFS."
https://www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2025.1746712/full

The meta-analysis by Kolala et al. (2025a) selected 12 studies and was set up to examine "whether a non-protocol based CBT is effective in a population ...
Autoantibody landscapes in neurological Long COVID and post-COVID cognitive impairment show heterogeneity without a shared disease signature — Debanjana Chakravarty et al
"Across tissue-based assays and peptide-level, whole-human-proteome PhIP-Seq profiling, the data consistently reveal a lack of convergent, disease-specific autoantibody signatures."
https://www.medrxiv.org/content/10.64898/2026.03.19.26348833v1

Background: Neurological Long COVID (n-LC) includes persistent cognitive and autonomic symptoms after SARS-CoV-2 infection. Prior studies of post-COVID conditions have described diverse humoral autoreactivity, but findings are heterogeneous, and it remains unclear whether n-LC is associated with a consistent CNS-directed humoral signature. Methods: We performed a cross-cohort case-control analysis to detect autoantibodies in cerebrospinal fluid (CSF) and serum from n-LC participants. In the Yale COVID Mind Study cohort, CSF from n-LC participants and from pre-pandemic and post-COVID asymptomatic controls was assessed by mouse brain immunofluorescence and proteome-wide phage immunoprecipitation sequencing (PhIP-Seq), with candidate reactivities evaluated by orthogonal assays and supervised modeling. In the Epidemiology, Immunology, and Clinical Characteristics of Emerging Infectious Diseases with Pandemic Potential (IDCRP EPICC) cohort, post-COVID sera collected prior to iPhone- or iPad-based cognitive screening were profiled by PhIP-Seq and compared between participants with and without cognitive impairment. Results: CSF immunoreactivity on mouse brain tissue was observed in both n-LC and controls, with similar overall frequencies, although n-LC participants more often showed nuclear-predominant staining patterns. PhIP-Seq identified sparse, largely patient-specific peptide reactivities to nuclear and neuronal proteins in CSF and serum. Supervised models provided limited discrimination between cases and controls. Candidate autoantigens had limited disease specificity on orthogonal testing. EPICC serum autoantibody profiling similarly failed to distinguish individuals with and without cognitive impairment. Conclusions: Across cohorts and compartments, n-LC did not exhibit a shared autoantibody signature. These findings support the absence of a dominant, common CNS autoantibody-mediated mechanism in n-LC. ### Competing Interest Statement SDP reports that the Uniformed Services University (USU) Infectious Diseases Clinical Research Program (IDCRP), a US Department of Defense institution, and the Henry M. Jackson Foundation (HJF) were funded under a Cooperative Research and Development Agreement to conduct an unrelated phase III COVID-19 monoclonal antibody immunoprophylaxis trial sponsored by AstraZeneca. The HJF, in support of the USU IDCRP, was funded by the Department of Defense Joint Program Executive Office for Chemical, Biological, Radiological, and Nuclear Defense to augment the conduct of an unrelated phase III vaccine trial sponsored by AstraZeneca. Both of these trials were part of the US Government COVID-19 response. Neither is related to the work presented here. MRW has received research-unrelated grant funding from Roche/Genentech, Novartis, and Kyverna Therapeutics, consulting fees from Ouro Medicines, Indapta Therapeutics, Vertex Pharmaceuticals, and Pfizer, and is a co-founder and on the Board of Directors for Delve Bio. ### Funding Statement This EPICC protocol was supported by awards from the Defense Health Program (HU00012020067 and HU00012120103) and the National Institute of Allergy and Infectious Disease (HU00011920111), the National Institute of Neurological Disorders and Stroke (R01NS125693) and the Westridge Foundation. The protocol was executed by the Infectious Disease Clinical Research Program (IDCRP), a Department of War (DoW) program executed by the Uniformed Services University of the Health Sciences (USUHS) through a cooperative agreement by the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. (HJF). The Yale COVID mind study was supported by National Institute of Mental Health (R01MH125737); National Institute of Allergy and Infectious Disease (R01AI157488); the National Institute of Neurological Disorders and Stroke (K23NS133488). This project has been funded in part by the National Institute of Allergy and Infectious Diseases at the National Institutes of Health, under an interagency agreement (Y1-AI-5072), and the National Multiple Sclerosis Society Postdoctoral Fellowship for DC. Sequencing was performed at the UCSF CAT, supported by UCSF PBBR, RRP IMIA, and NIH 1S10OD028511-01 grants. ### Author Declarations I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained. Yes The details of the IRB/oversight body that provided approval or exemption for the research described are given below: All studies in the Yale COVID Mind study cohort were approved by the Yale University IRB (HIC#1502015318), and written consent was obtained from all participants. All EPICC participants also provided informed consent, and the EPICC protocol was approved by the Uniformed Services University (USU) Institutional Review Board (Protocol number- IDCRP-085).The protocol was executed by the Infectious Disease Clinical Research Program (IDCRP), a Department of War (DoW) program executed by the Uniformed Services University of the Health Sciences (USUHS) through a cooperative agreement by the Henry M. Jackson Foundation for the Advancement of Military Medicine, Inc. (HJF). I confirm that all necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived, and that any patient/participant/sample identifiers included were not known to anyone (e.g., hospital staff, patients or participants themselves) outside the research group so cannot be used to identify individuals. Yes I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance). Yes I have followed all appropriate research reporting guidelines, such as any relevant EQUATOR Network research reporting checklist(s) and other pertinent material, if applicable. Yes All PhIP-seq data are available for download at Dryad and code is deposited in GitHub.
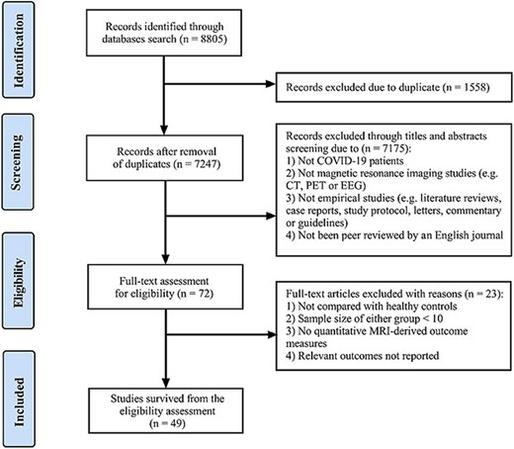
Widespread structural and functional brain alterations in COVID-19: a systematic review of MRI studies — Chen et al
"We identified 49 articles meeting the inclusion criteria." "We comprehensively summarized COVID-19 associated microstructural and functional alterations, categorized by imaging modality."
Cognitive and Neuropsychiatric Sequelae After SARS-CoV-2 Infection: A Narrative Review and Exploratory Cross-Sectional Study of Neurofilament Light Chain and GFAP — Crystell Guadalupe Guzmán Priego et al
"Nearly two years after infection, plasma NfL and GFAP concentrations did not differ between severity groups, indicating no detectable ongoing axonal or astrocytic injury at the group level."
Metacognition and cognitive dysfunction in post-COVID condition — Oliver-Mas et al
"In general, patients with PCC showed inaccurate judgments in both local and global metacognition compared to HC."
https://www.frontiersin.org/journals/psychology/articles/10.3389/fpsyg.2026.1786395/full
Paxlovid shows organ-specific and age-specific impacts on risk of developing post-acute sequelae of COVID-19 — Azhir et al
"We applied multivariable logistic regression with inverse probability weights to infer causal effects" "Overall, Paxlovid did not significantly reduce the risk of PASC across all age groups and organ systems."
Azhir, Cheng, et al use a validated electronic health record cohort and causal inference methods to assess the impact of Paxlovid on the risk of developing Long COVID. They find no overall reduction in risk, but observe fewer digestive symptoms and modest benefit in older, non-hospitalized adults.
Transfer of IgG from long COVID patients induces symptomology in mice — Hung-Jen Chen et al
"our study provides evidence for a pathogenic role of IgG in long COVID" "Cross-species constraints, such as hIgG-murine FcγR interactions and antigen orthology, may also influence pathogenic effects"
https://www.cell.com/cell-reports-medicine/abstract/S2666-3791(26)00110-2