🤔 Not what I expected!
More people preferred high diagnostic uncertainty than low, even though the higher uncertainty caused more worry.
Within- and between-subject, quant and qual results: https://doi.org/10.1136/jme-2024-109932
#medicine #decisionScience #probability #bioethics #openAccess
To what extent should doctors communicate diagnostic uncertainty with their patients? An empirical ethics vignette study
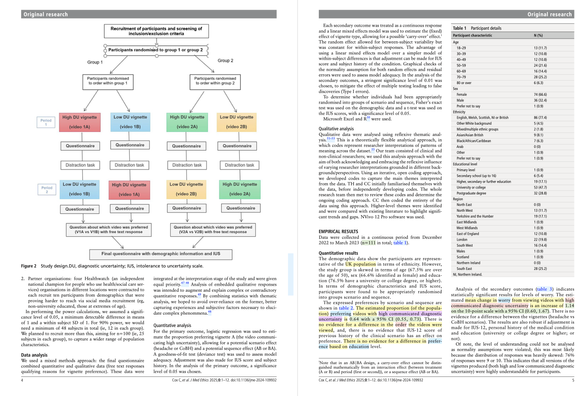
Background/aims Although diagnostic uncertainty is common, patient-focused research examining its communication is lacking. We aimed to determine patient preferences for the communication of diagnostic uncertainty, and examine the effects of such communication on patients. Methods We applied an empirical ethics approach, integrating the data collected with ethical analysis to form normative recommendations about diagnostic uncertainty communication. In this randomised crossover study, n=111 members of the public sequentially watched two video vignettes depicting either high or low communicated diagnostic uncertainty, in one of two clinical scenarios. After watching videos, participants completed online questionnaires. Primary outcome was preferred video (high vs low communicated uncertainty); secondary outcomes included satisfaction, trust, worry and understanding. Quantitative data were analysed using logistic regression and a linear mixed effects model; qualitative data were analysed thematically. Results Quantitative analysis demonstrated that participants preferred greater diagnostic uncertainty communication, even though these vignettes were more worrying. Qualitative data revealed heterogeneous participant views justifying their communication preferences. These data raise issues relating to how doctors might balance harms versus benefits in diagnostic uncertainty communication and how doctors might communicate in the face of heterogeneous patient information preferences. Conclusions We argue that doctors should err on the side of greater diagnostic uncertainty communication: to not do so (eg, based on benign paternalistic ideas about avoiding patient worry) or to do so variably (eg, based on unevidenced assumptions about patient information preferences) risks depriving patients of information they may value and may create or exacerbate inequalities. Data are available upon reasonable request. The participants of this study did not give written consent for their data to be shared publicly, only that the anonymised data collected may be used to support other researchers in the future. As such, the data that support the findings of this study are only available on request from the corresponding author, CC.