#TechniquetuesdayThis week we are highlighting ‘#Robotic
#Partial #Nephrectomy Course Tips for
#Retroperitoneal #Partial #Nephrectomy' by Dr. James Porter. Don’t forget to check out our video library of surgical technique videos in the StayCurrentMD app!
Full video:
https://youtu.pulse.ly/v8knmjzmyc#SoMe4PedSurg #PedSurgMade possible by Cincinnati Children's Hospital Medical Center
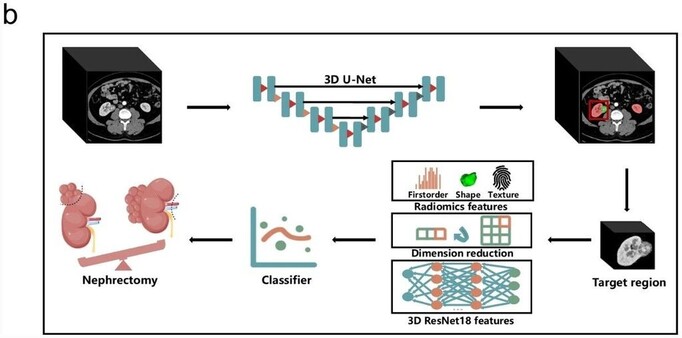
Proposed #automated analytic framework aims to assist #surgeons in partial or radical #nephrectomy decision-making. (Huancheng Yang et al.)
#EuropeanRadiology #OpenAccess
Read the full article here 👉 https://link.springer.com/article/10.1007/s00330-023-09812-9

An automated surgical decision-making framework for partial or radical nephrectomy based on 3D-CT multi-level anatomical features in renal cell carcinoma - European Radiology
Objectives To determine whether 3D-CT multi-level anatomical features can provide a more accurate prediction of surgical decision-making for partial or radical nephrectomy in renal cell carcinoma. Methods This is a retrospective study based on multi-center cohorts. A total of 473 participants with pathologically proved renal cell carcinoma were split into the internal training and the external testing set. The training set contains 412 cases from five open-source cohorts and two local hospitals. The external testing set includes 61 participants from another local hospital. The proposed automatic analytic framework contains the following modules: a 3D kidney and tumor segmentation model constructed by 3D-UNet, a multi-level feature extractor based on the region of interest, and a partial or radical nephrectomy prediction classifier by XGBoost. The fivefold cross-validation strategy was used to get a robust model. A quantitative model interpretation method called the Shapley Additive Explanations was conducted to explore the contribution of each feature. Results In the prediction of partial versus radical nephrectomy, the combination of multi-level features achieved better performance than any single-level feature. For the internal validation, the AUROC was 0.93 ± 0.1, 0.94 ± 0.1, 0.93 ± 0.1, 0.93 ± 0.1, and 0.93 ± 0.1, respectively, as determined by the fivefold cross-validation. The AUROC from the optimal model was 0.82 ± 0.1 in the external testing set. The tumor shape Maximum 3D Diameter plays the most vital role in the model decision. Conclusions The automated surgical decision framework for partial or radical nephrectomy based on 3D-CT multi-level anatomical features exhibits robust performance in renal cell carcinoma. The framework points the way towards guiding surgery through medical images and machine learning. Clinical relevance statement We proposed an automated analytic framework that can assist surgeons in partial or radical nephrectomy decision-making. The framework points the way towards guiding surgery through medical images and machine learning. Key Points • The 3D-CT multi-level anatomical features provide a more accurate prediction of surgical decision-making for partial or radical nephrectomy in renal cell carcinoma. • The data from multicenter study and a strict fivefold cross-validation strategy, both internal validation set and external testing set, can be easily transferred to different tasks of new datasets. • The quantitative decomposition of the prediction model was conducted to explore the contribution of each extracted feature.