 MD
MDHeadline result from the #Sparsentan PROTECT trial in #IgANephropathy in #Lancet https://authors.elsevier.com/c/1grIl_3CjG8WAP
1/🧵
Full text link via @Rheault_m
Big proteinuria reduction:
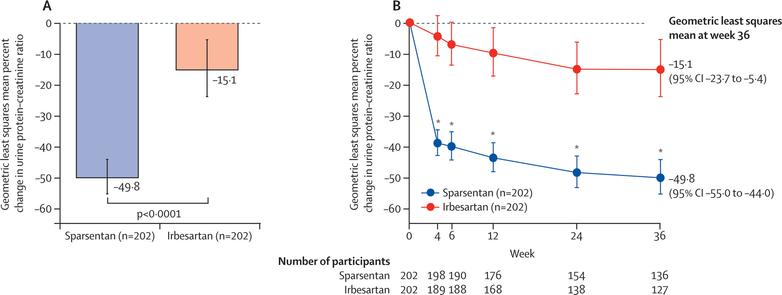
Headline result from the #Sparsentan PROTECT trial in #IgANephropathy in #Lancet https://authors.elsevier.com/c/1grIl_3CjG8WAP
1/🧵
Full text link via @Rheault_m
Big proteinuria reduction:
This is the methods section of interest - RASi ‘optimized’ ie the maximum tolerated dose had to be at least 50% of max (😏) and BP < 150/100
Note biopsy timing doesn’t matter
Note exclusion for heart failure (Endothelin antagonist specific issue!)
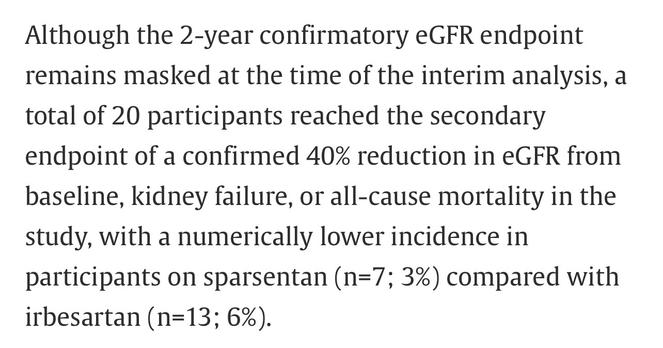
This is the interim result for FDA approval (obtained) of 36 week follow up, final follow up is 114 weeks, plus an observational period
2/


This is the other way of looking at proteinuria reduction - again pretty impressive
You may think - perhaps this is related to BP reduction with 400 mg Sparsentan vs 300 mg Irbesartan….?
3/
But you would be wrong
Hardly any difference in BP!
Hmm - maybe Endothelin blockade does something specific hemodynamically?
4/
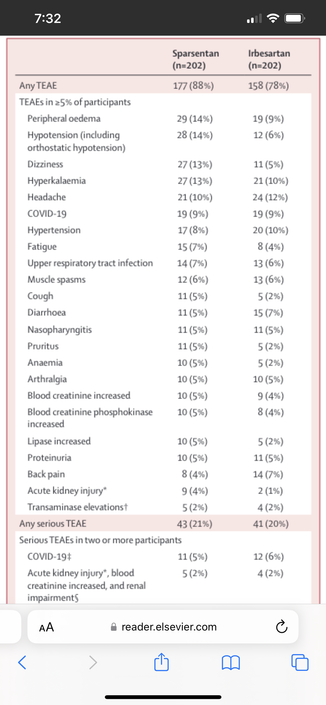
Adverse effects of interest - as expected more sodium retention and even more AKI (!) with #Sparsentan
The clinical kidney outcomes were less with Sparsentan (7 vs 13) but this is where I would like to see longer term effects of that sodium retention with Sparsentan. So let’s wait and see for final results I say
5/
Remiss in not showing table 1 - here it is
~ 40 years old
~ 70% men
~ 30% Asian
Just over a gram of proteinuria
GFR just under ~ 60
About 6+ years from biopsy - so mostly burnt out IgA like the Flozin trials?
6/
On the topic of flozins - no flozins allowed during double blind phase
🤷🏽♂️
My 2 cents: I am not using #Sparsentan - clearly flozins cheaper, with CV benefit. Sparsentan might reduce proteinuria but in long term cause CV harm.
Should we use them in combo? Maybe
7/7
Agreed. ERAs need to be combined with diuretics (Flozins, others, perhaps MRAs) - @ChristosArgyrop sez we should be doing this automatically (aka Cards combining ARNi with Valsartan)
Also:
- if Flozin/RASi/ERAs become standard baseline therapy, there will be less people remaining with 1 g proteinuria to qualify for the immunosuppression strategies. Is that wrong, as Sean Barbour pushed back on the podcast? https://podcasts.apple.com/ca/podcast/freely-filtered-a-nephjc-podcast/id1461664501?i=1000574598538
